Can the Face Actually Change in Adults?
Yes. That's the short answer, and it's the reason mewing and interoral facepulling took over the internet: thousands of people pushing on their own palate and reporting that their jaw, cheekbones, and midface shifted. The before-and-afters are real enough to be worth explaining.
The hypothesis underneath all of it is simple. The adult face isn't finished. It holds whatever position the forces around it ask for, and those forces can be changed.
There's a quieter proof of this that has nothing to do with any technique. Measured in 3D over time, the average adult face grows about 4% more asymmetrical every decade. It keeps moving on its own, dragged off-centre by years of uneven load. If everyday force can drift the face one way, deliberate force can guide it the other. What follows is why that's possible: how a skull that looks finished is still moving, and still movable.
Your Skull Is Not Fused Solid
Most people are told the skull fuses solid after puberty. It doesn't.
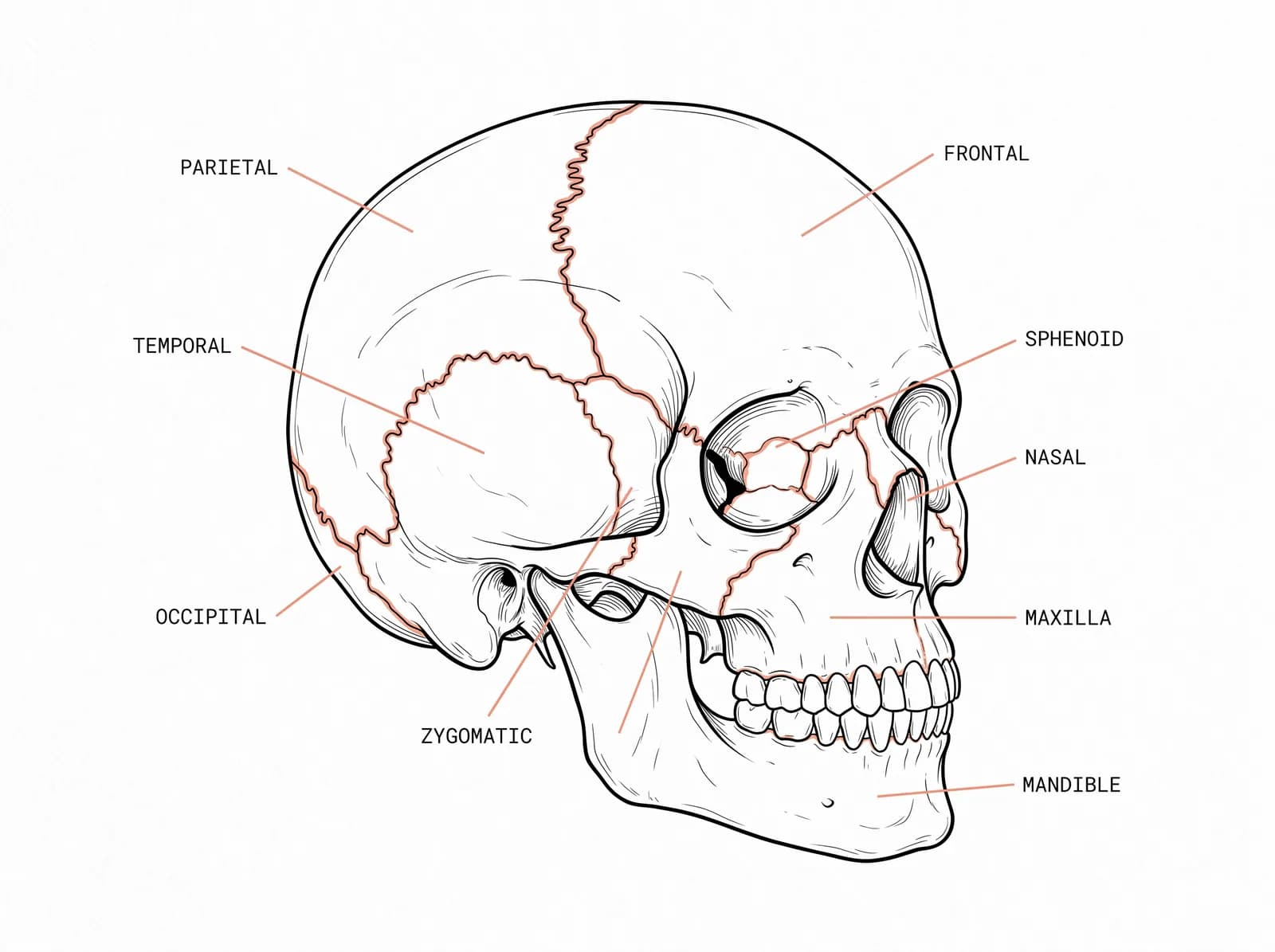
The adult skull is 22 bones, and all of them meet at sutures: fibrous joints that stay open and movable for most of your life. They don't fully close until the fifth to seventh decade, and often not even then. Inside those joints are blood vessels and nerve endings, which is how we know they're alive rather than scarred shut. Retzlaff found both still intact in the sutures of elderly cadavers.
The Craniosacral Rhythm
Those joints don't just allow movement. The cranial bones move all the time, in a slow, steady rhythm.
The membranes lining the skull, the fluid around the brain and spinal cord, and the subtle pull of the dura drive a continuous, rhythmic motion through the sutures. Osteopaths call it the craniosacral rhythm, or the primary respiratory mechanism: the skull quietly "breathes", expanding and contracting in a slow cycle. And it's measurable in living people, not just felt by hand. Moskalenko recorded the cranial dimensions of healthy adults shifting by about 0.4 millimetres each cycle, and Crow and colleagues caught the same calvarial motion on MRI, the skull's measured height and width changing over a few minutes of scanning.
This is the part that matters. The skull is not a finished object that locked into shape years ago. It's a living structure in constant gentle motion, which is exactly why its position can still be guided. Sustained, gentle, directional pressure across the suture lines, the basis of manual suture traction therapy, can over months nudge the bones toward a different resting position. Nothing is cut, dissolved, or rebuilt. This is repositioning, not added bone, which is the whole point of why you don't need more bone mass. The joints simply settle somewhere new.
Cranium to Sacrum: One System
The name craniosacral is literal. The skull and the sacrum are linked, top to bottom, by the dural membrane that runs the length of the spine and by the fascia that wraps everything in between.
So the cranial base doesn't sit in isolation. Tension lower down travels up. A tilted pelvis, a rotated atlas, a compressed spine, a habitual forward head, even how you load your feet, all pull on the same connected system and end up expressed at the top, in the face. The bite belongs to this chain too, since the teeth and the dental height help hold the skull level, and the skull and posture hold each other.
This is why chasing a single feature rarely works. One cheek, one eye, one side of the jaw is the visible end of a pattern that runs through the whole body. Work on the feature and you've worked on a symptom. The thing holding it there is the system underneath.
Soft Tissue Sets the Shape
There's a reason the same structure drifts over a lifetime: bone takes its shape from the forces around it. Moss called this the functional matrix. The tongue, the lips, the cheeks, the fascia, and the muscles of the jaw press on the skeleton constantly, and the bone holds the position those forces ask of it.
You can see it in how the midface forms. With every swallow the tongue presses up into the palate, which is the floor of the maxilla, hundreds of times a day. High, forward tongue posture guides the upper jaw forward and wide. Drop the tongue, breathe through the mouth, and eat food soft enough that nothing has to work, and the maxilla drifts the other way, down and back, taking the cheekbones and the airway with it.
The forces that built the face are the same ones holding its current shape. Change which forces win, sustained over time, and the structure has a reason to move.
What This Means for Reading Your Face
Your face isn't a fixed genetic output, and it isn't a single part that broke. It's the current position of a living, connected structure, set by years of uneven force moving through the whole system.
That cuts both ways. The position isn't permanent, but you also can't read it from one feature in the mirror. A cheekbone sitting high, an eye sitting low, a jaw pointing off-centre: each one is the surface of something running down through the cranial base, the bite, the spine, and the way the whole body is loaded. Seeing what's actually going on means looking at the system, not the symptom.
Sources
Park, Hwang, and Park (2022). Development of a Cranial Suture Traction Therapy Program for Facial Asymmetry Correction Using the New Delphi Technique. Medicina. A peer-reviewed, expert-validated protocol for applying gentle, sustained traction across the cranial sutures.
Moskalenko et al. (1999). Measured cyclic changes in the cranial dimensions of healthy adults of roughly 0.4 mm, evidence of continuous cranial motion in living people.
Crow, King, Patterson, and Giuliano (2009). MRI study capturing measurable calvarial motion in healthy adults.
Moss, the functional matrix hypothesis: bone form is maintained and modified by the soft-tissue forces acting on it.
Retzlaff, histological studies finding intact blood vessels and nerves within adult cranial sutures.